Mucous Membrane Grafting in Stevens – Johnson Syndrome
Dr. Prabhat Nangia, Dr. Sarang Lambat, Dr. Neha Shah, Dr. Vinay Nangia
Suraj Eye Institute, Nagpur, India
Introduction :
Stevens-Johnson syndrome (SJS) is an idiosyncratic reaction to drugs or infectious agents that leads to erythematous skin and extensive detachment of epidermis and mucous membrane erosions.1 Chronic ocular features include trichiasis, punctal scarring, limbal stem cell damage and lid margin keratinisation.2 These features lead to chronic debilitating ocular irritation, photophobia and blurred vision and do not respond well to conservative therapy.3
Case Details :
A female, 36 years of age, came to us with chief complaints of foreign body sensation, frequent blinking and photophobia in both eyes since 7 years. She had previously undergone right-sided dacryocystorhinostomy 7 years ago, following which she received some oral antibiotics and then developed skin rashes over face and torso along with redness of both eyes. She was treated locally as Stevens-Johnson syndrome and skin rashes resolved, however she then noticed severe foreign body sensation in both eyes. She consulted elsewhere and was treated with lubricants but felt no improvement. On examination best corrected visual acuity (BCVA) was 6/6p, N8 in right eye and 6/6, N6 in left eye. Slit lamp evaluation showed confluent patches of keratinization of all four lid margins (Fig. 1) along with trichiatic lashes. Multiple punctate erosions were seen over anterior surface of both corneas. Rest of the ocular examination was normal.
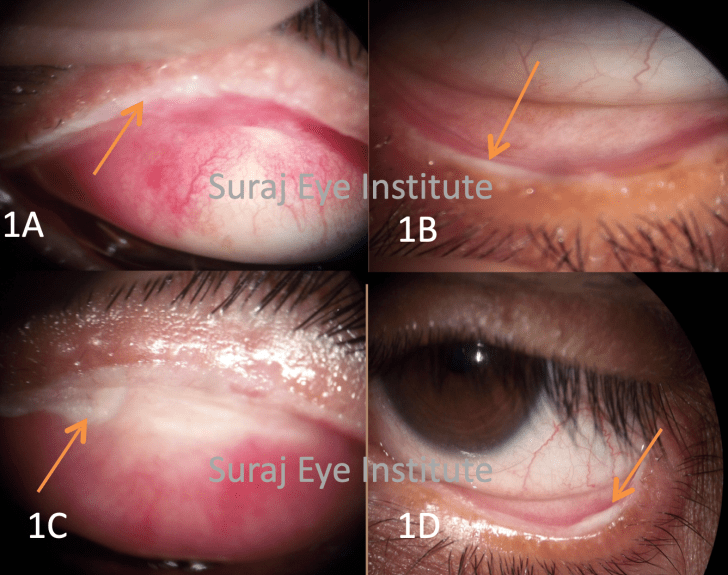
and lower lids (1D)
Management:
After removal of the trichiatic lashes, the patient was advised to undergo mucous membrane grafting (MMG) of all four lids. Keratinised conjunctiva was excised (Fig. 2A) and oral mucous membrane graft was harvested from lower lip mucosa (Fig. 2B) which was then trimmed by removing buccal fat (Fig. 2C) and then anchored to bare area using continuous 10-0 vicryl sutures (Fig. 2D), which were removed after one week. Oral mucosal wound was sutured with 7-0 vicryl. One month after surgery grafts were well apposed (Fig. 3), eyes were moist and there was significant improvement in her photophobia.


Discussion:
The tarsal ulceration that occurs during the acute phase of SJS leads to destruction of the muco-cutaneous junction of the lid margin, which is then replaced by overgrowth of the keratinised skin. Use of MMG to cover the bare area created by the excision of the keratinisation acts as a barrier preventing further growth of keratinised skin.2 MMG was found to improve the symptoms, BCVA and Schirmer 1 test values in SJS eyes.3 In view of the above, we decided to perform MMG and the patient felt significant symptomatic relief.
References :
1. Mockenhaupt M. Stevens-Johnson syndrome and toxic epidermal necrolysis:clinical patterns, diagnostic considerations, etiology, and therapeutic management. Semin Cutan Med Surg. 2014 Mar;33(1):10-6. Review doi: 10.12788/j.sder.0058.
2. Iyer G, Pillai VS, Srinivasan B, et al. Mucous membrane grafting for lid margin keratinization in Stevens–Johnson syndrome: results. Cornea. 2010 Feb;29(2):146-51 DOI: 10.1097/ICO.0b013e3181ae2691
3. Iyer G, Srinivasan B, Agarwal S, et al. Treatment Modalities and Clinical Outcomes in Ocular Sequelae of Stevens-Johnson Syndrome Over 25 Years—A Paradigm Shift. Cornea. 2016 Jan;35(1):46-50 DOI: 10.1097/ICO.0000000000000680