Vinay Nangia, Ravi Daberao
A CASE PRESENTATION:
A female 50 year of age, came for a follow up for glaucoma. Her best corrected visual acuity was 6/6 in right eye and 6/6 in left eye. Anterior segment examination was normal. Right eye intraocular pressure was 16 mmHg and left eye was 17 mmHg. She was on brimonidine tartrate (0.2%) and timolol maleate (0.50 %) combination eyedrops since 2 years. Gonioscopy showed open angles in both eyes. Her axial length in right eye was 21.89 mm and left eye 21.93 mm. Her central corneal thickness in right eye was 458 microns and left eye was 478 microns.

Figure 1B: Left eye color fundus photograph with a magnified view of the disc and RNFL.

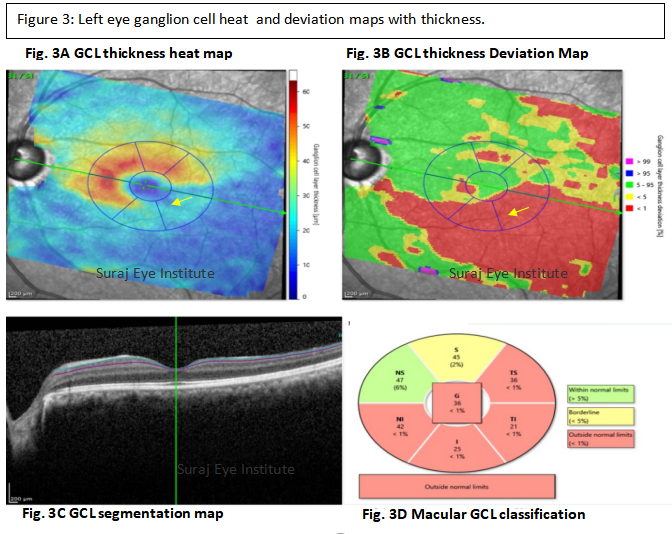

Impression: The patient presented to us with advanced glaucomatous damage in the left eye with significant retinal nerve fiber layer and ganglion cell layer thinning in the left eye. The intraocular pressure in the left eye was 17 mmHg with two anti-glaucoma medications. The CCT in the left eye was 478 microns which is relatively less than the normative values found in Central India. The patient was advised to use prostaglandins in addition to the current medications. It is important to note that over the last visit, there has been a loss in the superotemporal segment and superonasal segments. Loss may not be detectable in the inferotemporal segment, since there already exists significant damage leading to a flooring defect. In view of the significant and progressive glaucomatous damage, the option of surgery for glaucoma was also discussed with the patient.
PS. For the effect of central corneal thickness in the management of such a patient please read about GlacuomaLearn of the right eye.
Correspondence
Dr. Vinay Nangia
MS, FRCS, FRCOphth
Director
Suraj Eye Institute
Email – education@surajeye.org