Dear All:
I hope this find you all well. Imaging has taken centre stage in our lives as ophthalmologists and if it were to be a separate sub-speciality then it would perhaps be a very important one. The transition of our clinical senses and management to become dependant on images of the eye has been an important one. From the time, when just looking at the colour photos of the optic disc and the macula and the fluorescein angiography negatives, was the high point – to now, when nothing short of visualising each layer of the retina and each vessel in the retina is enough. Likewise anterior segment imaging has taken us into a new zone, as we try to see smallest of structures, that can make a difference to our diagnosis and clinical care and to our ultimate aim as ophthalmologists to give 6/6 vision to all our patients. We are pleased to bring you ImageWise a collection of images from cases that we hope will captivate your minds and hearts and drive you further in your careers.
Do enjoy yourselves.
Kind regards.
Vinay Nangia
Chairman- Suraj Eye Institute.
Pattern of retinal nerve fibre layer loss in a glaucoma patient
Dr. Shreya Jaiswal, Dr. Prabhat Nangia, Dr. Sarang Lambat, Dr. Vinay Nangia
Suraj Eye Institute, 559 New colony, Nagpur, India
Case Description
A male 57 years of age, came for a routine ophthalmic examination. He was a known case of systemic hypertension since 15 years and primary open angle in both eyes since 7 years. He was on topical brimonidine 0.2% and timolol 0.5% combination eyedrops twice daily in both eyes. His best corrected visual acuity was 6/6, N6 in both eyes. Anterior segment examination showed pseudophakia in both eyes. Intraocular pressure as recorded by Goldmann applanation tonometer was 16 mmHg in right eye and 18 mmHg in left eye.

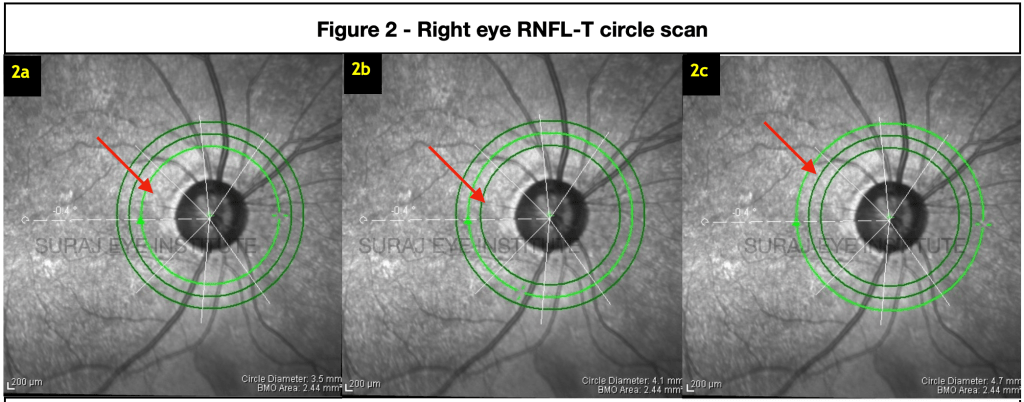
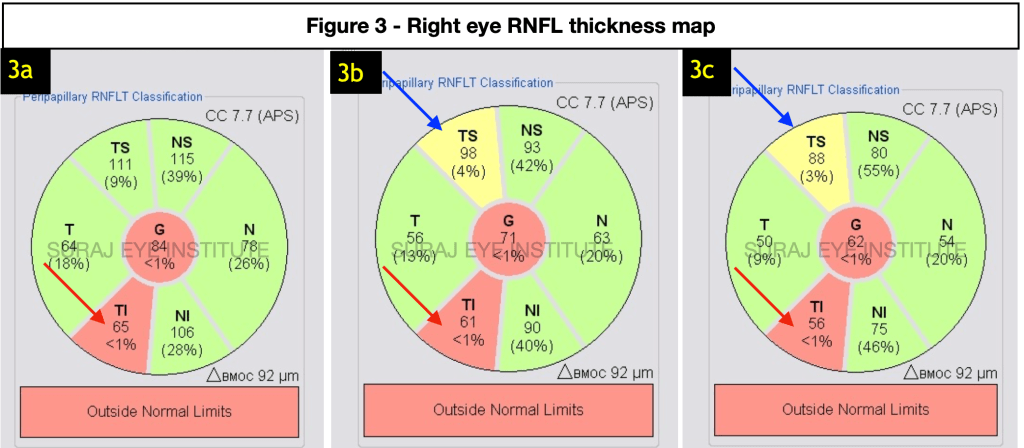
Figure 3b shows RNFL thickness at the 4.2mm diameter circle (figure 2b). There is appearance of RNFL thinning in the superotemporal quadrant (blue arrow) as the RNFL circle moves away from the disc.
Figure 3c shows RNFL thickness at the 4.7mm diameter circle. It shows further thinning of the superotemporal RNFL segment (blue arrow) and of inferotemporal segment (red arrow).
Discussion
With the advent of optical coherence tomography (OCT), cross-sectional imaging of the RNFL has improved the detection of RNFL damage. The RNFL thickness measurements has been largely limited to a 3.4 mm diameter circle around the optic disc. This case illustrates that there may be thinning of the RNFL that may not be visible in its early stages with the 3.4 mm diameter circle of the RNFL thickness determination. In some cases middle and outer circle RNFLT may help to diagnose early glaucoma and enable better follow up.
ReadWise
- Leung CK, Choi N, Weinreb RN, Liu S, Ye C, Liu L, Lai GW, Lau J, Lam DS. Retinal nerve fiber layer imaging with spectral-domain optical coherence tomography: pattern of RNFL defects in glaucoma. Ophthalmology. 2010 Dec 1;117(12):2337-44. https://doi.org/10.1016/j.ophtha.2010.04.002
Correspondence
Dr Vinay Nangia
MS, FRCS, FRCOphth
Director
Department of ophthalmology
Suraj eye Institute
Email –education@surajeye.org