Optical Coherence Tomography features of a retinal capillary macro-aneurysm
Dr. Shashank Somani, Dr. Sarang Lambat, Dr. Prabhat Nangia, Dr. Vinay Nangia
Suraj Eye Institute, 559, New Colony, Sadar, Nagpur- 440001.
Case Description
A male, 68 years of age, came with complaints of gradual progressive diminution of vision in the right eye, since 1 year. He was known case of diabetes mellitus and systemic hypertension since 35 years. His best corrected visual acuity was 6/12(p), N12 in right eye (RE) and 6/9, N8 in left eye (LE). Anterior segment examination showed presence of grade 1 nuclear sclerosis in both the eyes. Intraocular pressure recorded by Goldmann applanation tonometer was 10 mmHg in both eyes.
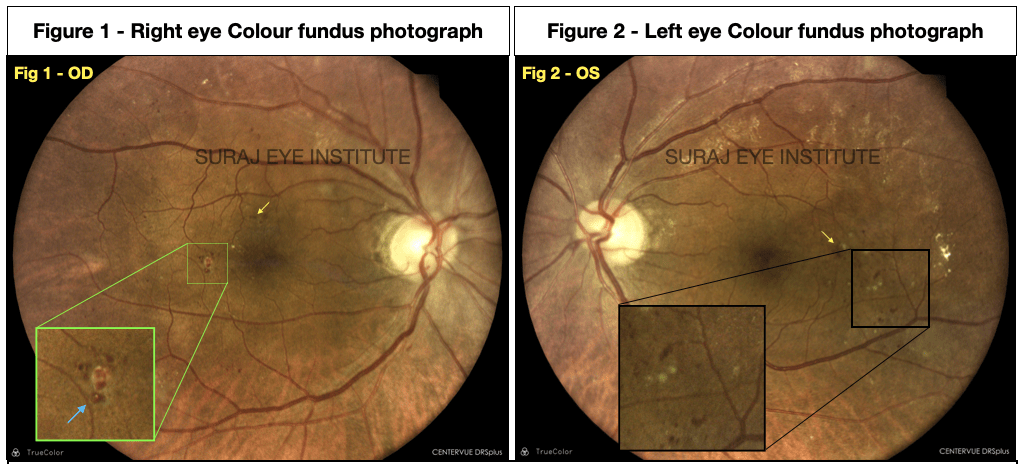
The highlighted part in Figure 2 (black box) shows multiple micro-aneurysms in the area temporal to fovea.




Figure 6a: Early arteriovenous phase in which we can see hyperfluorescence in the area of macro-aneurysm.
Figure 6b: Late arteriovenous phase showing multiple micro-anueysms and increase in the intensity of hyperfluorescence in the area of macro-aneurysm without any significant leakage. The cystoid macular edema can be seen in a faint petaloid appearance. (Green arrow)
Figure 6c: Recirculation phase showing minimal diffuse leakage from the macro-aneurysm
The patient was advised to undergo intravitreal inj Anti-VEGF in both the eyes followed by macular laser. The patient took injection in right eye on 20-11-20.

Discussion
Retinal capillary macroaneurysms (RCMs) are considered to be solitary outpouchings from the retinal capillaries and are distinct from the capillary micro aneurysm and retinal artery macroaneurysm (RAMs). One of the study, the aneurysms found in central retinal vein occlusion were noted to have a maximal diameter of 65 ± 39 microns and that in diabetic retinopathy to be 100 ± 57 microns. In contrast the size of RAMs ranges from 100 – 250 microns. There are 2 factors which facilitate enlargement of RCMs, one is decreasing wall strength and other is increasing wall tension. When these 2 factors come in play the lesion grows larger and leads to expansion of the RCMs.
Generally the RAMs are present in the inner retinal layers but RCMs are present in the outer retinal layers and was associated with minimal intraretinal fluid adjacent to the macro-aneurysm. Intervention may be required in cases of exudative or hemorrhagic macro-aneurysms. Different modalities of treatment include Laser photocoagulation or Anti-vascular endothelial growth factor therapy have been described for RAMs. Photocoagulation is known to produce coagulative necrosis of cells and coagulation of the blood within the RCM and it was shown to involution of the lesion and resolution of the leakage. In this case the macro-aneurysm was relatively silent and was not causing any damage to the surrounding retina however there was a presence of cystoid edema in the macular area for which the patient was advised injection Anti-VEGF followed by macular laser.
Our patient showed an irregular shaped macro aneurysm clinically on the fundus photograph. (Fig. 1) There was also presence of white tissue surrounding the macro aneurysm specially in the superior half. The presence of fibrosis may be indicative that this aneurysm may not be ‘active’ and is unlikely to cause significant associated retinal pathology. A hint of fibrosis may also be visible in Fig. 3 (yellow arrow). The appearance of the macro aneurysm on the FFA ( Fig 6 b) gives a beaded appearance which may also be suggestive of fibrosis setting in. This can only be a good sign, in that it may indicate a ‘macro-aneurysm in resolution’. In this patient however there were multiple microaneurysms indicate of significant diabetic maculopathy resulting in macular oedema as seen in the images above.
ReadWise:
- Spaide RF, Barquet LA. RETINAL CAPILLARY MACROANEURYSMS. Retina. 2019 Oct;39(10):1889-1895. doi: 10.1097/IAE.0000000000002406. PMID: 30489449.
- Amoroso F, Pedinielli A, Colantuono D, Jung C, Capuano V, Souied EH, Miere A. Selective Photocoagulation of Capillary Macroaneurysms by Navigated Focal Laser. Ophthalmic Surg Lasers Imaging Retina. 2021 Jul;52(7):366-373. doi: 10.3928/23258160-20210628-02. Epub 2021 Jul 1. PMID: 34309425.
Dr. Sarang Lambat
MS, FRF
Consultant
Vitreoretinal services
Suraj Eye Institute
Nagpur
Email – education@surajeye.org