Sub retinal fluid in a case of age related macular degeneration
Dr. Samyak Gupta, Dr. Sarang Lambat, Dr. Prabhat Nangia, Dr. Vinay Nangia
Suraj Eye Institute, 559, New Colony, Sadar, Nagpur- 440001.
Case Description
A male, 59 years of age, came with a complaint of distortion of vision in right eye, along with a black spot since 6 months. He had a history of oral carcinoma for which he was on treatment. His best corrected visual acuity(BCVA) was 6/6 P, N8 in right eye (OD) and 6/6 P, N6 in left eye (OS). Anterior segment examination showed early cataract in both eyes. Intraocular pressure recorded by Goldmann applanation tonometer was 10 mm Hg in both eyes.

Figure 2: Fundus photograph of the left eye showing the presence of drusen (white arrow).


Patient was advised to undergo intravitreal anti-VEGF injection in right eye. He initially opted for Inj. Bevacizumab. Patient was followed up monthly post each injection. At his follow up visit after the fifth intravitreal anti VEGF injection, his OCT scans showed presence of a choroidal neovascular membrane along with subretinal fluid. As the lesion still persisted after multiple Bevacizumab injections, he was switched over to Inj. Ranibizumab.

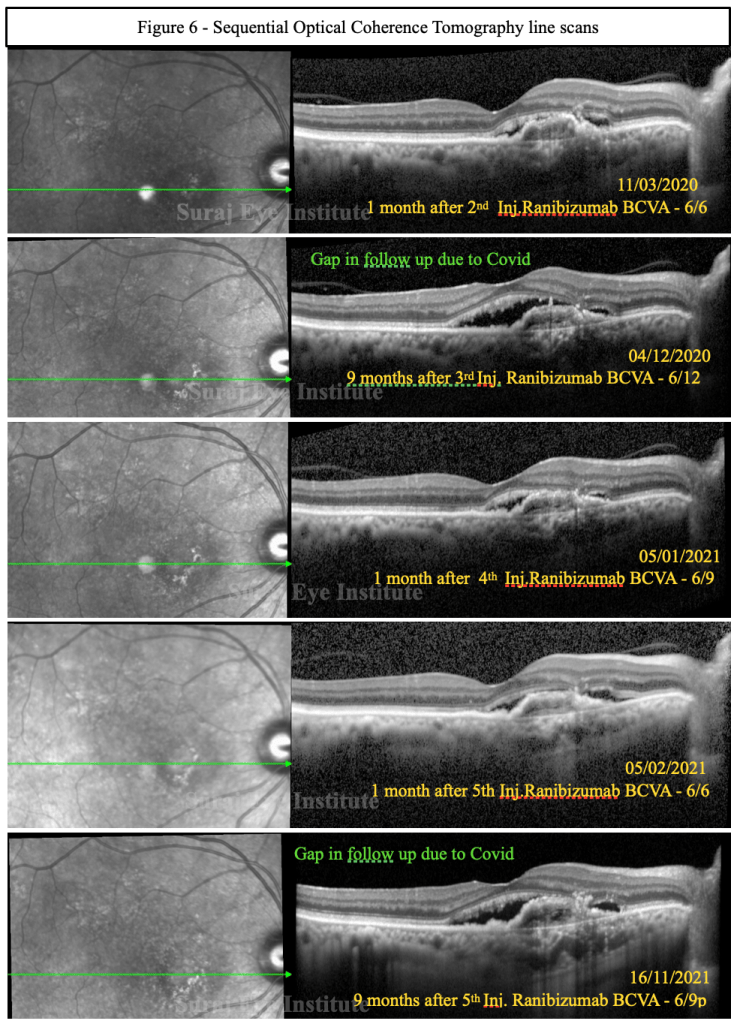
Figure 6b shows colour fundus photograph of right eye at 3 months follow up. The view of the fundus was not as clear as on one month because of development of grade 2 nuclear sclerosis cataract in the right eye. There is growth of epiretinal membrane as shown in a comparison of increased tortousity (red arrowheads) of blood vessels in Fig. 6a and 6b.


After almost 5 injections of ranibizumab there was persistence of SRF in the right eye. He was given the option of a longer acting anti VEGF molecule, to reduce the need of frequent injections. Patient was advised Inj. Brolucizumab which he underwent in the right eye subsequently. On his follow up visit 2 weeks after the injection, OCT scans of right eye showed the complete resolution of SRF.

Discussion
In our case, patient presented with subretinal fluid(SRF) in right eye with Type 1 CNV (Figure 3). SRF is a very important OCT biomarker in AMD and it is the only OCT biomarker which is a good prognostic indicator.
Our patient showed the persistence of SRF despite regular Inj. Bevacizumab, possibly due to the development of tachyphylaxis. Hence we switched to Ranibizumab for further 5 injections. Unfortunately there was persistent SRF despite regular injections. Subsequently there was a gap in the follow up twice due to the two waves of Covid pandemic and his systemic condition. Considering his situation we offered him long acting anti-VEGF, Inj Brolucizumab. Patient was willing for the injection but he developed recurrence of his oral cancer and didn’t follow up for few months. Post injection he showed complete resolution of SRF.
In this case the patient presented with only SRF without any intraretinal fluid (IRF). It has been suggested that active CNVM should be treated before development of IRF. IRF indicates a long standing fluid and further delay in treatment in its presence leads to irreversible neurosensory damage. It is also observed that patients with subretinal fluid derive larger visual acuity benefits from anti-angiogenic treatment. In addition, eyes with SRF are less likely to develop RPE atrophy even under an intensive monthly anti-VEGF regimen. These eyes are also resistant to treatment but that does not affect the final outcome. In this patient patient maintained a good visual acuity (6/18) despite long course of treatment. Patient has also developed visually significant cataract and has also been advised surgery for the same. It is also important to note that the drying effect of brolucizumab is much better than other agents. (Fig 8)
Several anti-VEGF agents are available for ocular use including Bevacizumab, Ranibizumab, Brolucizumab, Aflibrecept etc. Tachyphylaxis has been noted to occur with the use of Inj Bevacizumab and Ranibizumab. It has been observed that compared to other agents Inj Brolucizumab is less costly and more cost-effective than Aflibercept and Ranibizumab.
ReadWise:
- Kent JS, Iordanous Y, Mao A, Powell AM, Kent SS, Sheidow TG. Comparison of outcomes after switching treatment from intravitreal bevacizumab to ranibizumab in neovascular age-related macular degeneration. Canadian Journal of Ophthalmology. 2012 Apr 1;47(2):159-64.https://doi.org/10.1016/j.jcjo.2012.01.003
- Yu JS, Carlton R, Agashivala N, Hassan T, Wykoff CC. Brolucizumab vs aflibercept and ranibizumab for neovascular age-related macular degeneration: a cost-effectiveness analysis. Journal of managed care & specialty pharmacy. 2021 Jun;27(6):743-52. https://doi.org/10.18553/jmcp.2021.27.6.743
Dr. Sarang Lambat
MS, FRF
Consultant
Vitreoretinal services
Suraj Eye Institute
Nagpur
Email – education@surajeye.org