Bruch’s membrane, trauma and myopia
Dr. Shashank Somani, Dr. Sarang Lambat, Dr. Prabhat Nangia, Dr. Vinay Nangia Suraj Eye Institute, 559, New Colony, Sadar, Nagpur- 440001.
Case Description
A male, 20 years of age, presented with blurring of vision in left eye (LE) since 10 years. He gave history of trauma to the Left eye 10 years back. On examination his best corrected visual acuity (BCVA) was 6/6, N6 in right eye (RE) and 6/36p, N36 in the left eye (LE). The refraction in RE was Plano and in the LE it was -10DS/ +1.75DC x 30. On slit lamp examination, RE anterior segment examination was normal. The left eye showed the presence of mild patchy cataract suggestive of post traumatic lenticular changes. His intraocular pressure (IOP) was 12 mmHg in RE and 10 mmHg in LE. Axial length of RE was 25.42mm and LE was 28.83mm. The keratometry in right eye was k1 = 40.56D / 8.32mm @ 26 and k2 = 41.46D / 8.14mm @ 116 and in LE was k1 = 40.18D / 8.40mm @144 and k2 = 41.16D / 8.20 mm @ 54.

Figure 2: Fundus photograph of LE shows presence of a large crescentic scar running across fovea which is concentric to the disc, showing significant atrophic changes (blue arrow) and intervening RPE proliferation (green arrow). This was suggestive of a choroidal tear. Another crescentic area of RPE atrophy concentric to the optic disc, located along the temporal margin of the disc is seen suggestive of a second choroidal tear. (Pink arrow). An area of relatively normal retina can be seen between the disc and the second choroidal tear which differentiates it from a gamma zone or peripapillary atrophy. (Black arrow)







Discussion
Our patient presented with poor vision in the left eye. On retinal evaluation, there was presence of a concentric area of parapapillary atrophy. Of interest was the presence of an area of seemingly normal appearing retina between the optic disc and the area of atrophy. The patient is highly myopic in the LE, with a refractive error of -10 DS and an axial length of 28.83 mm. Therefore one may have assumed that there would be an area of parapapillary atrophy normally seen in high myopes. However there is no typical parapapillary area of myopia, but there is an area as mentioned above of circumlinear atrophy away from the optic disc. This area has developed due to the blunt trauma suffered by the patient at the age of 10 years.
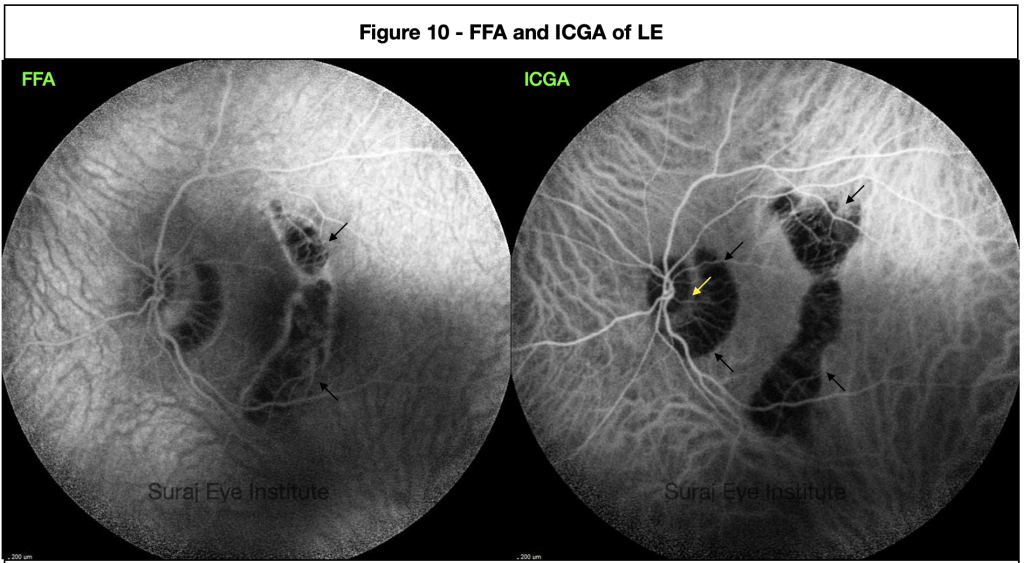
Temporally there is another almost concentric vertical oriented area of atrophy cutting across the fovea. This area shows the presence of a choroidal tear ( Figures 6b blue arrow, 8b blue and red arrow, and 9b blue arrows) with associated herniation of the retinal layers in the cup made of the sclera posteriorly and the choroid on the sides. Choroidal tears are classically seen in blunt injury and are often associated with significant loss of vision specially when they involve the fovea as in our case. They are also associated with the development of choroidal neovascularization, which further decreases vision depending on the site of development.
While the literature alludes to these changes as a choroidal tear, we would like to think it may be more scientific to consider these as Bruch’s membrane tears, which they are. The choroid is damaged but a typical break is seen in the Bruch’s membrane as in our patient. Further Bruch’s membrane breaks are classically and more often associated with the development of a choroidal neovascularization as also seen in a myopic CNV and in age related macular degeneration.
The Bruch’s membrane has often been associated with changes that are typical of myopia. Thus elongation of the eye with an associated increase in axial length is related to the development of a Gamma zone which is the space between the clinical optic disc margin, mostly the temporal margin, and the margin of the Bruch’s membrane opening. One may presume that the Bruch’s membrane has moved away from the original clinical margin of the optic disc due to the axial elongation. Our patient did not give a history of myopia, poor vision or of wearing glasses in childhood. While we are aware that media opacities in childhood can result in axial length increase with associated myopia, macular changes in childhood resulting in decreased vision are not specifically known to be associated with axial length increase. The Bruch’s membrane is thought to be produced in the retro equatorial region resulting in increased axial length. While that is a considered mechanism for normal eyes, our patient had a Bruch’s membrane break due to trauma, that was in some areas 2000 microns wide.
Our patient had high myopia with a significantly increased axial length. At least from the history it was evident that myopia was not preexistent before the development of the Bruch’s membrane tear. There is therefore a possible explanation for the increased axial length, that it may have occurred due to the break in the Bruch’s membrane. It is possible that because of the Bruch’s membrane break the layers of the eye may have moved and stretched, allowing a significant increase in axial length to occur. It would be most helpful if there were more cases to study, however such a unique happenstance is a significant opportunity to elucidate the mechanism behind myopia in our patient.
ReadWise
- Jonas JB, Ohno-Matsui K, Jiang WJ, Panda-Jonas S. Bruch membrane and the mechanism of myopization: a new theory. Retina. 2017 Aug 1;37(8):1428-40. doi: 10.1097/IAE.0000000000001464
- Moon K, Kim KS, Kim YC. A case of expansion of traumatic choroidal rupture with delayed-developed outer retinal changes. Case Reports in Ophthalmology. 2013;4(2):70-5. https://doi.org/10.1159/000354197
Dr Vinay Nangia
MS, FRCS, FRCOphth
Director
Suraj Eye Institute
Email – education@surajeye.org
QuizWise
Q. 1 – Which of the the following are true.
- The Bruch’s membrane is thicker than the retinal pigment epithelium
- The Bruch’s membrane is considered and hypothesised to have a role in axial length increase
- The Bruch’s membrane is a stretched firm membrane that does not develop folds.
- The Bruch’s membrane opening is does not match the clinical margins of the optic disc in emmetropia.
Q. 2 – Which of the following are true and found in association with a choroidal tear following blunt trauma
- The anterior segment will always be normal
- There may be development of CNV.
- There is no loss of vision following a choroidal tear
- Choroidal tears are always associated with a retinal detachment.