SIMPLE LIMBAL EPITHELIAL TRANSPLANTATION
Dr Prabhat Nangia, Dr Sarang Lambat, Dr Vinay Nangia
559, Suraj Eye Institute, Nagpur.
Case Description
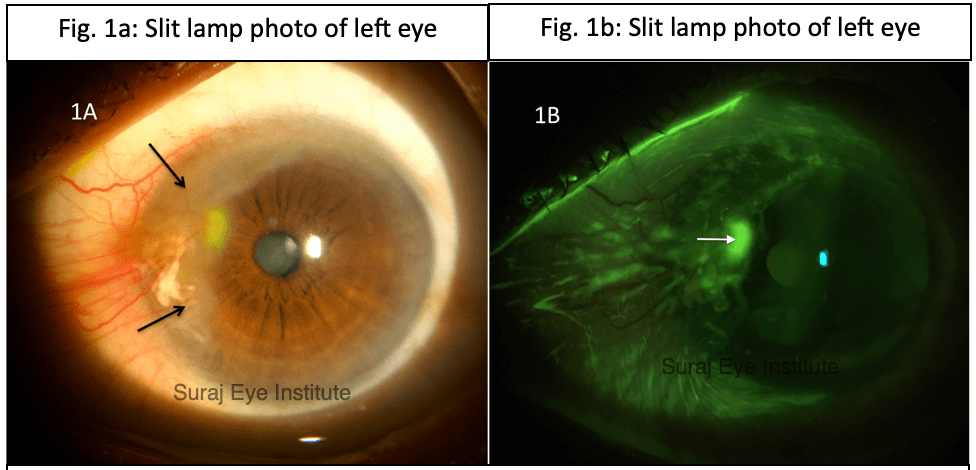
A male, 65 years of age, came with chief complaints of pain and redness in left eye (OS). There was no history of left eye surgery, trauma or chemical injury. Patient did not have any symptoms of rheumatological disorder. Best corrected visual acuity was 6/24,N36 in right eye (OD) due to the presence of a choroidal neovascular membrane at the macula. On slit lamp examination, OD was within normal limits. There was a pseudopterygium in OS in the nasal and superonasal area from 7 to 12 o’ clock, where the conjunctiva had grown over the cornea (Fig. 1A). The pseudopterygium had an inflamed surface with an overlying epithelial defect (Fig. 1B), which was resulting in the eye pain and redness.
The patient was advised topical steroids and lubricants for symptomatic relief. However, he was keen on permanent resolution of the symptoms, which would entail removal of the inflamed pseudopterygium. We decided to combine this with a simple limbal epithelial transplantation (SLET) by harvesting limbal epithelial cells from OD. A 2 by 2 mm area of the limbus in the superonasal quadrant of OD was dissected carefully and the limbal cells were kept in balanced salt solution prior to further dissection. The pseudopterygium was dissected off the cornea and sclera, and the bare area was covered with amniotic membrane which was stuck to the surface with fibrin glue. The limbal cells were divided into 6 to 7 SLET ‘bits’, which were placed over the amniotic membrane, and a drop of each component of fibrin glue was placed over the SLET bits. A bandage contact lens was then placed over the cornea, to prevent the SLET bits from falling off.
On first post operative day, the SLET bits were seen in situ, close to the limbus (Fig. 2).

Three weeks later, the surface epithelium had healed completely, with establishment of corneal phenotype over the entire area. The SLET bits were seen as before. There was no surface inflammation (Fig. 3 A and 3 B).

The final follow up was 8 months post operatively, and the SLET bits were seen hazily, suggesting that the epithelial stem cells from the bits had spread across the surface, leading to complete and sustained establishment of corneal phenotype (Fig. 4A and 4B). The patient was asymptomatic in OS.

Discussion
Limbal stem cell deficiency (LSCD) can result in blindness in one or both eyes and has a poor prognosis for penetrating keratoplasty. The use of limbal stem cell transplants first started with the advent of CLAU (conjunctival limbal autografting) wherein two donor lenticules (three clock hours each) of limbus and adjacent conjunctiva were harvested from the unaffected eye in patients with unilateral LSCD, and these were then transplanted to the eye with LSCD. While effective, this could result in iatrogenic LSCD in the donor eye. To prevent this, CLET (cultivated limbal epithelial transplantation) was introduced, which entailed harvesting one to two clock hours of limbal stem cells from the donor eye, which could then be ‘grown’ into a sheet of epithelial cells ready for transplantation to the eye with LSCD. This technique, while mostly successful in avoiding iatrogenic LSCD in the donor eye, requires a stem cell laboratory to cultivate the epithelial cells, which is difficult to set up and expensive. The advent of SLET,(1) which involves cultivation of the epithelial cells on amniotic membrane after transplantation, ensured that the advantages of CLET are retained without the regulatory or monetary hurdles.
Autologous SLET (stem cells from other eye of patient) has been used for multiple indications that may lead to unilateral LSCD- ocular surface burns, LSCD post ocular surface tumour excision, recurrent pterygia and others. In patients with bilateral LSCD, allogeneic SLET(2) (limbal stem cells from a cadaver eye or from a live donor) can be performed, but these cases will require systemic immunosuppression, to prevent graft failure.
Our patient had a pseudopteryium of unknown origin, with close to 5 clock hours of LSCD. While conjunctival autograft alone is a viable option in such eyes, we felt that SLET would allow us to preserve most of the ocular surface tissue in the contralateral eye, as such eyes would require a relatively larger conjunctival autograft. The SLET bits were successful in re epithelising the cornea and controlling the ocular surface inflammation within 3 weeks after the surgery. No complications were noted in the post operative period.
It is important to note that the underlying cornea should be relatively clear, so that there may be significant visual gain after the SLET. Otherwise, this procedure may need to be combined with a corneal transplant to achieve the desired outcome. However, concomitant penetrating keratoplasty may increase the chance of failure of SLET in these eyes.
ReadWise
- Sangwan VS, Basu S, MacNeil S, Balasubramanian D. Simple limbal epithelial transplantation (SLET): a novel surgical technique for the treatment of unilateral limbal stem cell deficiency. Br J Ophthalmol. 2012 Jul;96(7):931-4
- Shanbhag SS, Patel CN, Goyal R, Donthineni PR, Singh V, Basu S. Simple limbal epithelial transplantation (SLET): Review of indications, surgical technique, mechanism, outcomes, limitations, and impact. Indian J Ophthalmol 2019;67:1265-77
Correspondence
Dr Prabhat Nangia
DNB, FICO, FMRF, FAICO
Consultant
Department of Cornea and Ocular Surface
Suraj eye Institute
Email – education@surajeye.org
- Which of the following is an absolute contraindication for SLET?
- Blind eye with no visual potential
- Dry keratinised ocular surface
- Partial limbal stem cell deficiency
- Both a and b
2. Which of the following statements regarding SLET is false?
- Limbal stem cell deficiency in the donor eye is rare
- It cannot be repeated from the same donor eye
- It requires expensive stem cell laboratories
- Both b and c